Reading Glasses. These are glasses with convex lenses that
are used only for reading. By making the light rays less divergent,
these glasses reduce the amount of accommodation required and
lessen the likelihood of a ciliary spasm developing. If strong
enough lenses are selected, all the accommodation
can be eliminated and the eyes will be completely focused for
distance. Figure 2 shows how this happens, using an emmetropic or
normal eye as an example.
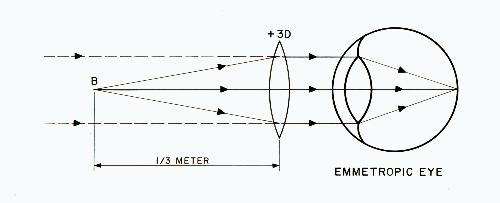
Fig. 2
Suppose that the book is normally held at about a distance of
one-third meter from the eyes, at B. Since a +3 D lens has a focal length
of one-third meter, if it is placed in front of the
eye it will make the diverging rays become parallel before entering
the eye. The dotted lines show that the eye is receiving parallel
rays as if from a distant object. Thus, this eye can read without
accommodation. This is called reading at the far point.
To better understand this idea, imagine that you wish to take
a picture of a close object using a camera that is focused for
infinity. You could do this and still get a clear picture if you
place a plus lens of appropriate power in front of the camera lens.
We are doing something similar with the eyes.
Now suppose that the book is pushed just a little farther away
from the eyes so that it becomes a little blurred. Figure 3 shows
this situation.
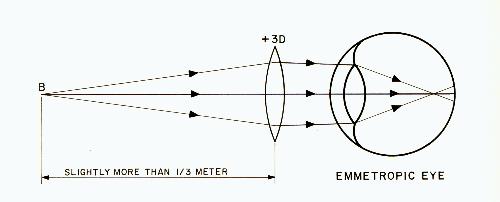
Fig. 3
Now the eye is receiving converging rays, something which
does not normally occur in everyday life. Only optical lenses make
this possible. Notice that the lens of the eye is fully relaxed and
cannot relax further. The rays are therefore bent too much and
come to a focus slightly in front of the retina. The result is a
slightly blurred image. This is called the blurred image or fogging
technique because it purposely makes the vision a little blurred or
foggy. This technique is especially useful in relaxing a ciliary
spasm that is already present. However, in dealing with an eye that
is already myopic, the true situation would be like figure 4 rather
than figure 3.
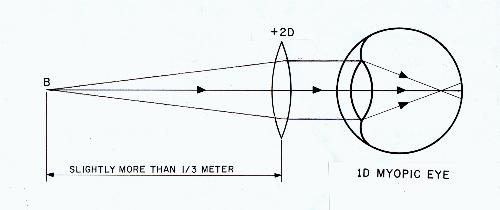
Fig. 4
Figure 4 represents an eye that is already rather myopic so that
even in its totally relaxed condition it requires diverging rays to
see clearly. If the eye is 1 D myopic, this means that it has + 1 D
more refractive power than it should have. Therefore, an additional
+2 D lens is all that is needed to give a total power of +3 D and
completely relax the eye for a one-third-meter reading distance.
The above reasoning can be expressed in tabular form as follows:
| Distance Prescription |
Reading Glass Lens Needed to Totally Eliminate Accommodation at 1/3 Meter Reading Distance |
| 0 |
+3 D |
| -1 D |
+2 D |
| -2 D |
+1 D |
| -3 D |
0 |
| -4 D |
-1 D |
| -5 D |
-2 D |
| -6 D |
-3 D |
The appropriate lens for each eye is selected individually since
the two eyes do not always have the same refractive error. However,
if the eyes are not too different in refractive power, the same
eyeglass lens power can be used for each eye without difficulty.
A special prescription for reading purposes is frequently called an
add since the distance prescription is used as the starting point
and the prescription for the reading glasses is added to it. To
illustrate, if a person uses -5 D lenses for distance and has a +2 D
add for reading, the reading prescription is -3 D.
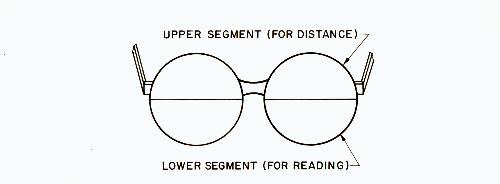
This terminology is most commonly used with bifocals (see
below) where the lower segment is the add. However, the same
terminology can be used if the add is a separate pair of reading
glasses.
The use of the fogging technique creates an active relaxation
of the ciliary muscle and thus has
a greater effect on relaxing a ciliary spasm than could be
accomplished by merely eliminating the accommodation (with no
fogging). The reason for this is that the ciliary muscle is composed
of two separate sets of fibers. The circular fibers are obviously
used to tighten the muscle and increase the accommodation. The
radial fibers are used by the eye to relax the muscle and decrease
the accommodation. This has been given the term negative
accommodation.
Thus, the fogging technique forces the ciliary spasm to relax,
as the eyes attempt to see the blurred image clearly. However, most
doctors who prescribe reading glasses do not give an add that
will eliminate all of the accommodation. They may prescribe an
add of only +1 D, +1.5 D, or +2 D. The reason for this is that
many children have difficulty "accepting" a large add. That is, the
add causes some "side effects" in the form of various vision
problems.
This drawback of reading glasses is due to the fact that there
is a strong linkage in the human visual system between accommodation
and convergence (turning the eyes inward when looking at
something close). As a viewed object approaches the eyes,
accommodation and convergence increase in proportion to each other.
Over thousands of years, the brain has learned that this is the
normal situation. Consequently, accommodation stimulates
convergence and vice versa. Thus, if we converge without
accommodating the appropriate amount, or if we accommodate without
converging the appropriate amount, problems can develop.
This close relationship between accommodation and convergence
is upset when reading glasses are used to eliminate the
accommodation for reading. Since the eyes must still converge
on the book, an unnatural situation is created. The result can
be eye fatigue, double vision, or other types of fusion problems.
That is, the two images can no longer be fused together without
discomfort. Normal binocular vision is interfered with. For this
reason, the book should be held as far as possible from the eyes to
reduce the amount of convergence needed.
This problem can also be partially overcome by prescribing
a prismatic component in the reading glasses to reduce the amount
of convergence required. Figure 5 shows how this is done.
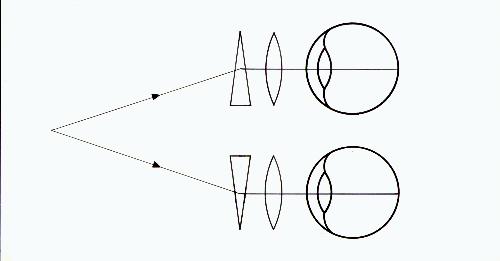
Fig. 5
These prisms are placed with the bases toward the nose and
are called base-in prisms. In figure 5, the plus lens and the prism
are shown separately. In reality they are made as one lens.
However, using prisms as described above to totally eliminate
convergence will cause severe distortion due to the
thickness and shape of the lenses, and is not done.
Reading glasses can also be made in a half-eye form in which
it is possible to look over the top of the lenses for distance
vision rather than having to remove the glasses.
The reading glasses with plus lenses that have been described
are the same type of glasses that usually become necessary for
people after they reach their forties. Because of changes in the
eyes with increasing age, the eyes can no longer accommodate
sufficiently for reading. Therefore, plus lenses are used by older
people because they can't accommodate; on children, plus lenses are
used to avoid accommodation. Reading glasses can be purchased
cheaply in many retail outlets. However, such reading glasses are
intended for adult-size heads. The distance between the lens centers
conforms to the usual distance between the pupils of adult eyes,
around 60mm when reading. If such glasses are used by young children,
who have a smaller interpupillary distance, the "prismatic effect"
of the lenses causes increased convergence. This can cause problems
such as double vision and should be avoided. The optical centers of
the lenses should be no further apart than the child's interpupillary
distance when reading.